We’re talking about key exercises for lower back pain. In the previous article we outlined some critical concepts to set the stage for why creating focused, individualized motion at the lumbar joints is critical. Now we need to move into the exercises themselves.
We’re going to start with focusing on exercise prescription for those patients that are in a lot of pain. These patients are classified as being “movement sensitive”. The hallmark here is that the patient has pain with basic movement testing.
This is a big deal. If the body isn’t able to perform basic movements it will impact the patient’s ability to fully participate in life’s required and desired pursuits. And if not treated properly this can also have significant long term consequences for the movement system that increase the risk of the condition becoming chronic or recurrent.
For example, pain with basic movement and tissue loading will lead to altered motor patterns and muscle activity. This is a motor response to reduce load on the affected tissue. This can come in the form of subtle alterations in muscle recruitment or patterning, muscle spasm or hypertonicity, or in more extreme cases antalgia.
In the short term some of these changes may be advantageous, but when prolonged can have significant consequences by limiting the adaptability of the movement system (see Rethinking Faulty Movement Patterns).
So clearing this sensitivity and building movement tolerance needs to become the top priority.
Do Pain Mechanisms Matter?
Of course when it comes to pain there may be different mechanisms at play. With acute injury an inflammatory reaction should be suspected. Here tissue swelling along with the accumulation of inflammatory mediators and other noxious chemicals will sensitise the receptors at the site of injury. These will be the patients who present with an obvious mechanism of injury. A fall, lifting injury, or MVA for example.
In other cases neuroplastic changes or altered CNS processing may be the primary pain mechanism. Here symptoms will be more longstanding and a specific MOI is unlikely. Or if there was a specific event that initiated the symptoms, the timeline has long exceeded typical and expected timelines for tissue healing.
Of course these are two simplified examples. In the real-world most patients will come to your office with more complicated and less obvious presentations. Recurrent pain or significant symptom flare-ups with no obvious MOI (like just waking up with acute pain?) come to mind here. (We talked more about the complexity of pain in our Rethinking Pain article series.)
But here’s the critical point….
Even though the mechanisms driving the pain itself may be different the treatment approach (at least from an exercise prescription approach in terms of what movements and exercises are most beneficial) is really not different. Certainly there will be subtle nuances in programming, and patient messaging needs to be tailored to each individual. But to me the initial focus still needs to be on developing tolerance to basic spine motion. And for this the exercises and movements we prescribe will be the same.
The Exercises: Pelvic Tilts for Pain and Movement Tolerance
We know movement is a powerful stimulus to control symptoms and guide tissue healing with acute pain and injury. But to be effective this movement needs to be directed at the right area. As discussed in the previous article, this is a major limitation with many traditional lower back stretches and exercises.
This is where pelvic tilts come in.
Because the lumbar spine sits atop the sacrum, tilting the pelvis anterior and posterior will create obligatory flexion and extension of the lumbar intervertebral joints in a bottom up sequence. Likewise side-to-side tilting will create lateral flexion and rotation through this same area.
Safety First
But to be effective the movements must also be safe and the patient needs to be able to control the symptom response. This is critical because in most cases of acute lower back pain almost any movement directed at the lower back will create symptoms. So patients may be fearful or reluctant to perform these or any other exercises.
Here again we see the effectiveness of pelvic tilts. Because these are non-weight bearing exercises they minimize the overall compressive forces on the spine. So tissue stress is relatively low. Any symptoms with these movements will be more related to tissue sensitivity as opposed to further damage or injury.
Move to tolerance – It’s not no pain no gain!
That is not to say we just push through pain. The instruction to patients is to “move to tolerance”. Some symptoms are OK, and even expected in the initial stages. But working into these symptoms can help reduce pain and swelling. Explaining to patients that symptoms here are more about tissue swelling and the accumulation of chemicals at the site of injury, and that movement helps push and flush these chemicals out of the area is powerful messaging here.
Here’s a detailed description of how to perform the specific exercises.
The exact tissue doesn’t really matter
Of course identifying a specific tissue of origin for most lower back pain is difficult. Not only do various tissues present with similar history and pain patterns, but they are also stressed with similar movements. For example, flexing the lumbar spine creates tension at the posterior aspect of the intervertebral discs, interspinous ligaments, joint capsules, various deep and superficial muscles, and spinal nerve roots.
But I don’t think this really matters that much. At least not from the perspective of what exercises the patient needs to perform. The fact is that all of these tissues (including nerves) need and respond well to movement as a stimulus for health and healing.
That’s why these pelvic tilt movements can be applied to virtually any type of lower back pain. Of course the specific symptom response may be different. Some conditions may be more sensitive with extension. Others with flexion. And some patients may demonstrate symptoms in both directions. But when these movements cause pain my primary objective becomes clearing these motions.
If the spine cannot perform basic non-weight bearing motion then clearing these movements becomes the top priority.
Movement and chronic pain
The above discussion really focused on acute pain and injury. But these same pelvic tilt exercises are a great starting point for chronic back pain as well.
Of course, acute pain is different from chronic pain. While an inflammatory response may driving the symptoms following injury, long standing pain is often related to a hyper-sensitive pain system. Here the CNS recognizes movement as unsafe and potentially threatening. It is as if the brain has “learned” that a movement is unsafe or potentially threatening. In an effort to protect the body the CNS calls upon the pain system. (We talked about this in more detail in our Rethinking Pain series.)
Here pain serves as a powerful modifier of behavior. A preemptive strike to limit exposure to what is believed to be a potentially dangerous or damaging event.
So where do pelvic tilts fit in here?
Recall that one of the key attributes of pelvic tilts is that they create focal individualized spine motion while minimizing load. So again, we know these movements are safe and any symptoms will be more related to tissue sensitivity as opposed to further damage or injury.
This is powerful messaging that can help the patient understand that pain is not always related to tissue damage. Even though the movements may create some pain, nothing bad happens. It helps the CNS to recognize the movement as less threatening. Over time, as the brain starts to trust the movement it can turn down the hyper-active pain system.
Quadruped Pelvic Tilts / Progressions
Pelvic tilts performed from a supine position as outlined above are my go-to option to improve pain and movement tolerance. But I also prescribe pelvic tilts from a quadruped position as soon as the patient can tolerate these movements.
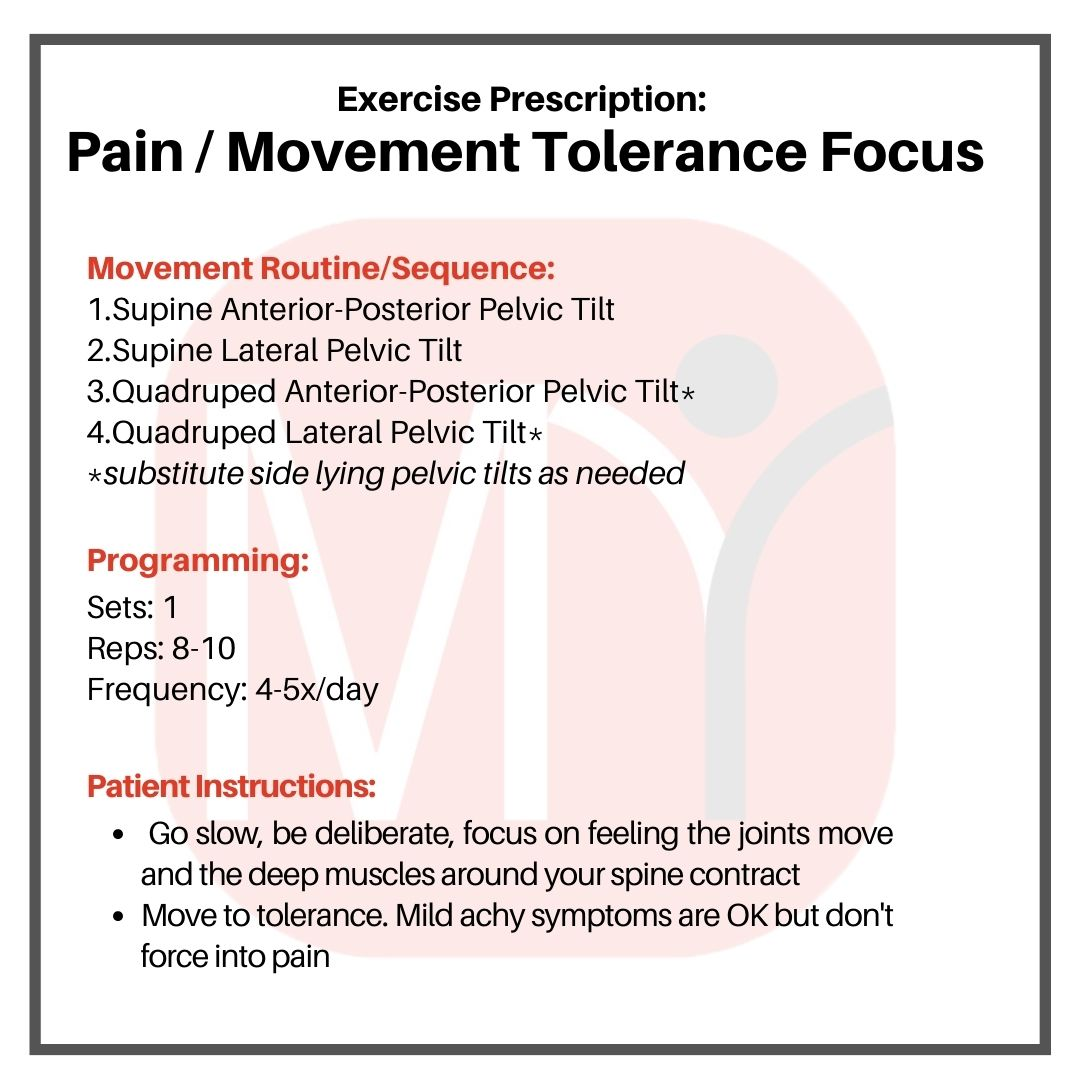
Exercise Programming
When improving pain and movement tolerance is the primary focus I want patients doing these exercises just a little a time. So we create a short movement routine consisting of 8-10 slow, deliberate repetitions of each movement. But I want the exercises done frequently. So this movement routine is repeated 4-5 times each day.
And remember, we don’t want our patients to just mindlessly go through the motions. We need them to be slow and deliberate with each repetition. They need to focus on feeling and visualising the motion as it occurs and concentrate on generating tension in the deep muscles of the spine to generate the movement.
Pelvic Tilt Regressions
There will be some patients who cannot tolerate the quadruped position. For these patients I substitute side lying pelvic tilts.
Make Exercise Prescription Easier with MRC
As simple as these exercises are there is a lot of information that goes with them. Form is critical. And so is understanding what to expect with respect to symptom response during the movements. Of course reviewing this directly with your patient is necessary, but providing a means for your patient to reference this information and the proper execution of the exercises from home is also critical.
To help with this all of these exercises are part of the My Rehab Connection library. (The instructional videos used here are the videos from the exercise library.) So you can easily prescribe these to your patients and give them easy home access through our free app or from a web browser.
If you are already a subscriber (if you’re not you can find out more about our program here) you can search for these exercises individually. But to make it easier I have created an Exercise Group titled “Low Back: Basic Movement Sequence: Pain/Tolerance Focus.” And don’t forget you can assign the entire group to your patient with a single click then remove or inactive any exercises that you don’t want then currently doing.
Up Next.. Part 3. Exercises For Mobility And Control
So that acute back pain. Up next is how to apply these principles to general/mechanical low back pain. These are the patients where “things just don’t work quite right”. The focus here needs to be (at least at first) on developed adequate mobility and control of the spine. Here is the link to Part 3.