
Part 1: Re-thinking The Traditional View of Pain
At first glance pain seems like a straightforward process. You stub your toe or break a bone and it hurts. This is how most people understand pain. It’s consistent with the patho-anatomical view that holds tissue damage or pathology as the source of pain.
Of course, few would dispute that tissue injury can and typically does result in pain, but a big problem occurs when we try to apply this model too broadly and make the assumption that all pain is related to tissue pathology, or alternatively, that all tissue pathology leads to pain. This is simply not supported in the clinical or pain science literature.
It’s Not Always About Injury or Damage
We see countless examples where imaging studies demonstrate tissue damage and pathology such as disc protrusions, annular tears, and arthritic joints in the absence of pain or other aberrant symptoms. More extreme examples can be found in reports in which soldiers experience gunshot wounds in battle yet feel no symptoms.
These are examples in which tissue injury or pathology is present in the absence of symptoms. But we also see many examples where patients experience pain with no discernable tissue damage or injury. Phantom limb pain is an example. Here we have individuals who have lost a limb due to injury or amputation, yet feel what is often described as excruciating and debilitating symptoms in the absent limb.
And of course as clinicians and therapists we have all seen pain that extends long past known healing times for tissue injury. In these cases tissue damage may be the initial instigator of pain, but the patho-anatomical model has trouble explaining why these symptoms remain long after the damage has healed.
Are Faulty Movement Patterns to Blame?
As the role of structural pathology with respect to pain and support for the patho-anatomical model began to wane, the focus shifted from a structural to a functional paradigm. Instead of how things looked on an x-ray or MRI, the focus turned to how things worked. The central tenet here was the idea that many common musculoskeletal conditions and their associated symptoms were the result of poor or suboptimal movement patterns.
Clinicians subscribing to this view (the kinesio-pathological-movement model, or KPM) – hold that improving and correcting these so-called faulty or compensatory movement patterns is a critical and necessary part of care.
This sounds enticing and is an easy sell on the surface, but the KPM also has it’s problems. Perhaps the biggest and most glaring issue is knowing and agreeing on what these so-called “faulty” movements are. Proponents of this model suggest there is an optimal way in which the body is designed to move to prevent injury and maximize performance. But is there actually a best/right way to move? Or is the variability of movement patterns and strategies seen across patients simply reflective of varying adaptive patterns of the complex, dynamic, biological system that is our body?
“Faulty” Movements Don’t Always Lead to Pain
The other elephant in the room is the fact that if these faulty patterns are in fact a cause of pain we would therefore expect to see a predictable relationship between these undesirable patterns and presenting symptoms. But this relationship is a difficult one to establish both in clinical practice as well as in the injury literature.
Take hyper-pronation for example. The image below depicts what appears to be a horrific case of hyperpronation. But this foot belongs to elite distance runner Joseph Cheptegei. Instead of leading to a life of injury and agony this foot has propelled Cheptegi to an illustrious running career, breaking 3 world records in 2020 alone.
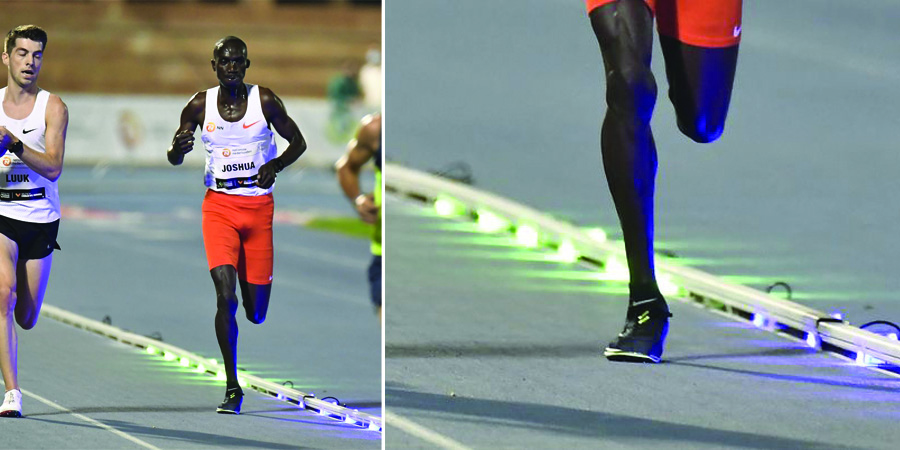
We’ve all heard of the perils of this sinister and debilitating condition that is hyper-pronation. Yet over and over we see examples of this so-called faulty and compensatory hyper-pronation both in clinical practice and in high-level athletics in individuals who seem to otherwise be doing just fine
Of course, this is an anecdotal report. A sample of one from an elite athlete with superhuman abilities. An outlier. Surely these observations do not apply to the general population. What about a more in depth analysis of the literature? What does the research have to say about the relationship between how we move and how we feel?
Let’s look at knee pain as a specific example.
Biomechanics and Knee Pain?
Patellofemoral pain syndrome (PFPS) is typically thought to be associated with a valgus malalignment of the knee. This “faulty’ alignment is believed to result from inadequate strength or motor activity of the posterior-lateral hip musculature (specifically the gluteal muscle group). So treatment is often focused around correcting knee mechanics by strengthening the hip.
But is this view supported in the literature?
At first glance it may appear so. With a quick article search we see numerous studies that consistently demonstrate hip weakness in the presence of PFPS (1-7). But does this weakness actually lead to faulty movement at the knee as has been suggested? Here the findings are less clear.
For example, Bolga et al. (2008) found no differences in lower extremity kinematics in subjects with PFPS despite differences in hip strength.
Other studies do report altered kinematics of the lower extremity with hip muscle weakness (2,19), but these changes are not consistent across groups. For example, both Souza et al. (2009) and Nakagawa et al. (2008) found females with hip muscle weakness also demonstrated greater magnitudes of hip internal rotation. However, these same results were not found in male subjects. Furthermore, while Nakagawa reported increases in hip adduction, Souza found no differences in hip adduction between PFPS and control groups.
So while patients with PFPS may demonstrate hip muscle weakness, exactly how this weakness affects pain and movement is not as clear as conventional beliefs suggest.
Establishing Cause Vs. Effect
But the tenuous relationship between strength and kinematics is not even the main issue. The more significant elephant in the room is that all these studies compare subjects who currently have PFPS with healthy controls. These cross-sectional designs provide no way to determine causation. They cannot tell us if the weak hip (or the “faulty movement that results) is the cause or the effect of knee pain.
It’s the chicken versus the egg debate.
We know that pain affects sensory-motor reflex arcs associated with the execution and control of movement. So it is plausible that increased nociceptive drive in the presence of knee pain leads to hip muscle weakness through neurologic motor inhibition.
Support for this can be found in a study by Park et al. (2017) who studied the effects of experimentally induced knee pain on hip muscle activation. Following injection of a hypertonic solution into the infrapatellar fat pad the authors reported a reduction in gluteus medius activation during a landing task, concluding that experimental knee pain leads to hip muscle inhibition.
Determining Cause Vs Effect
To determine whether gluteal weakness/knee valgus is a cause of PFPS we need to look at prospective/cohort studies. Unlike cross-sectional studies, prospective studies seek to measure variables of interest in a population before they develop a given condition. They seek to determine prospective risk factors for developing a certain condition of interest.
So if hip muscle weakness is in fact a significant causative factor in PFPS we would expect these prospective studies to bear this out. But this is not what we see.
Thijis et al. (2011) measured hip strength in healthy female athletes prior to the initiation of a running program. Of the 77 subjects who took part in the study 16 developed PFPS. However there were no differences in initial hip strength between these subjects and those who remained healthy.
Other prospective studies have not only failed to demonstrate hip weakness as a risk factor in knee pain, but in some cases have actually shown that individuals with greater hip strength are more likely to develop PFPS (10,11). Two recent in-depth systematic reviews also echo these conclusions, suggesting there is little evidence to support the notion that hip strength is a risk factor for PFPS (13,14).
So the commonly held belief that hip strength plays a pivotal role in lower extremity alignment, and that this alignment is a significant contributor to pain and injury at the knee appears to be much less clear than when studied on a deeper level.
Strengthening the Hip Reduces Knee Pain
But here’s where things get really interesting…
When we look at clinical studies in which the intervention focuses on exercises to strengthen the hip and improve dynamic alignment of the knee, these studies seem to consistently show improvements in PFPS (1-4).
For example, Tyler er al. (2006) and Khayambashi et al. (2012) studied the effects of exercise programs aimed at improving hip abduction and external rotation in subjects diagnosed with PFPS . Both studies concluded that following the program subjects reported significant reductions in pain. Furthermore, these reduced pain scores were accompanied by increases in hip muscle strength.
So on the surface it appears that increases in hip strength do in fact lead to improvement in PFPS. But the problem with this conclusion is, again, there is no way to infer causation. Yes we can say the intervention was effective in reducing knee pain, but to say that increases in hip strength lead to improvements in pain is beyond what these studies can tell us. Perhaps it was the other way around. Maybe the reduction in pain was responsible for the improvement in hip function?
This confusing relationship between hip strength and knee pain is further seen in studies by Dolak et al. (2011) and Nakagawa et al. (2008). Here we again see improvements in knee pain following a hip exercise program. In fact, both studies concluded subjects who performed hip exercises reported far greater improvements compared to subjects who performed exercises that were solely targeted at the knee.
But the interesting finding here is that despite improvements in knee pain, there were no improvements in actual hip strength. So if hip strengthening exercises reduce knee pain but don’t improve hip strength, what are the mechanisms or mitigating factors that are driving improvement?
What About Kinematics?
What about kinematics? Maybe these hip exercises have a bigger effect on the movement pattern. Maybe it is a reduced valgus orientation of the knee that is responsible for the improvements in knee pain?
Here we can look at an article by Saad et al. (2018) who compared the effects of an exercise program aimed at strengthening the hip against exercises aimed at the knee. Here we do see an improvement in hip strength in the hip exercise group that is not seen in the knee group. But when we look at knee kinematics (measured here as the number of subjects who demonstrated a knee valgus pattern with a step down task) we do see improvements in the hip group, but these improvements are no better than those seen in the knee group. In fact, there was a trend towards greater improvement in the knee exercise group.
So here we see improvements in both pain and kinematics, but these changes are not specific to the hip exercise group or do not seem to be driven by changes in hip strength.
So again this begs the question, what is driving these changes?
Re-thinking Pain in Terms of Modern Pain Science
So pain is not a straightforward process. The failures of the patho-anatomical and the KPM models to explain why we hurt clearly demonstrates pain does not follow a straightforward cause-effect relationship. There must be other factors at play that influence the quality, intensity, location, and duration of pain beyond the classical view that pain is synonymous with tissue injury or mechanical overload.
While we still don’t have all the answers, a significant body of work has emerged over the past few decades that has helped provide valuable insight into at least a few of these mysteries. In this article series we are going to explore some of these findings in an effort to provide a more modern and comprehensive view of pain.
To be clear, this does not necessarily mean completely re-working our treatment approach. Stretching and exercise prescription (and yes, manual therapy) still play a valuable role in the treatment of pain. But some changes are needed.
Coming Up Next…
Here in Part 1 we began by discussing the shortcomings of the traditional view of pain. Up next we’ll shift our attention to the critical role the brain plays in pain experience. Including an evolutionary perspective of the importance of pain why our ancient ancestors would need a pain system that is prone to hyper-sensitivity.
References
- Tyler et al. (2006). The role of hip muscle function in the treatment of patellofemoral pain syndrome. Am J Sports Med, May.
- Nakagawa et al (2008). The effect of additional strengthening of hip abductor and lateral rotator muscles in patellofemoral pain syndrome: a randomized controlled pilot study. Clin Rehabil, 2008 Dec;22(12):1051-60.
- Khayambashi et al. (2012). The effects of isoloated hip abductor and external rotator strength on pain, health status, and hip strength in females with paterllofemoral pain: A randomized controlled trial. JOSPT, 2012; 42 (1).
- Dolak et al. (2011). Hip strengthening prior to functional exercises reduces pain sooner that quadriceps strengthening in females with patellofemoral pain syndrome: A randomized controlled trial. JOSPT, 2011; 41 (8).
- Saad et al. (2018). Is hip strengthening the best treatment option for females with patellofemoral pain? A randomized controlled trial of three different types of exercise. Brazilian J Physical Therapy, 2018; 22 (5): 408-416.
- Bolga et al. (2008). Hip Strength and knee kinematics during stair descent in females with and without patellofemoral pain syndrome. JOSPT, 2008; 38 (1).
- Robinson and Nee. (2007). Analysis of Hip Strength in Females Seeking Physical Therapy Treatment for Unilateral Patellofemoral Pain Syndrome. JOSPT, 2007; 37 (5): 232-8.
- Souza et al. (2009). Differences in hip kinematics, muscle strength, and muscle activation between subjects with and without patellofemoral pain. JOSPT, 2009, 39
- Park et al. (2017). Effects of Experimental Anterior Knee Pain on Muscle Activation During Landing and Jumping Performed at Various Intensities. J Sport Rehabil, 2017 Jan;26(1):78-93
- Finnoff et al. (2011). Hip strength and knee pain in high school runners: A prospective study. PMR, 2011; 3 (9): 792-801.
- Herbst et al. (2015). Hip Strength Is Greater in Athletes Who Subsequently Develop Patellofemoral Pain. Am J Sports Med. 2015 November ; 43(11): 2747–2752
- Thijis et al. (2011). Is hip muscle weakness a predisposing factor for patellofemoral pain in female novice runners? A prospective study. Am J Sports Med, 2011; 39(9): 1877-82.
- Rathleff et al. (2014). Is hip strength a risk factor for patellofemoral pain? A systemic review and meta-analysis. Br J Sports Med, 2014, 4; 48(14): 1088.
- Neal et al. (2018). Risk factors for patellofemoral pain: A systematic review and meta-analysis. Br j Sports Med, 2018.
More from my site
 PAIN: A Modern View On Why We Hurt (Part 2: Pain and the Brain)
PAIN: A Modern View On Why We Hurt (Part 2: Pain and the Brain) PAIN: A Modern View of Why We Hurt (PART 3: Fear, Learning, and Pain)
PAIN: A Modern View of Why We Hurt (PART 3: Fear, Learning, and Pain) PAIN: A Modern View of Why We Hurt (PART 4: Operant Conditioning and Pain)
PAIN: A Modern View of Why We Hurt (PART 4: Operant Conditioning and Pain) Pain: A Modern View On Why We Hurt (Part 5: Treatment Considerations)
Pain: A Modern View On Why We Hurt (Part 5: Treatment Considerations) 5 Steps To Improving Mobility – Part 1
5 Steps To Improving Mobility – Part 1 Super Simple Hamstring Exercise Progression
Super Simple Hamstring Exercise Progression