Follow My Rehab Connection on Instagram @MyRehabConnect
Acute low back pain is a common presentation in health care clinics. Fortunately, the majority of cases respond well to conservative care. But appropriate early intervention is important to increase the chances of recovery. This is particularly true with home exercise prescription. Not only can the right exercises help control pain and promote tissue healing, but they can also give patients a sense of control over their condition.
But what are the best exercises for acute low back pain? Prescribing home exercise as early as possible (hopefully on the first visit) is preferred. However, we must be careful to prescribe exercises that are simple, effective, and will not exacerbate their symptoms.
The Best Exercises For Acute Low Back Pain
All tissues need to move. Even painful and damaged tissue. Think of a muscle injury. Obviously if we overuse the injured muscle it will create further damage. But not moving the muscle can be just as bad. This can lead to additional tissue stiffness and can cause inflammatory mediators to accumulate, leading to nociceptor sensitization and abnormal vascular responses.
The same thing is true with acute low back pain. Whether it is a damaged or irritated joint, disc, muscle, ligament, or even a nerve root, the rules are the same. The tissues need to move to promote healing and reduce pain. But they need to move the right way and the right amount. Too much movement can flare up the condition and has the potential to create further damage. This is not what we want to do with acute back pain patients who are already anxious about the condition.
So the question becomes, what are the best exercises for acute low back pain? How can we promote a safe about of movement that will help reduce pain and encourage tissue healing? The answer is… pelvic tilts.
Why Pelvic Tilts Work
I have found pelvic tilt exercises to be the best exercises for the vast majority of these patients (but only if done correctly, as discussed below). Here’s why…
As the pelvis rocks back and forth it creates a oscillating flexion-extension motion of the lumbar spine. This helps to mobilize the lumbar joints and restore normal vertebral motion. These gentle oscillations also create cyclical interstitial pressure changes within the muscles and passive tissues of the spine. These changing pressure gradients help to flush any build up of inflammatory exudates out of the area.
But while pelvic tilts can be one of the safest and most effective exercises for low back pain, to be most effective they must be done correctly. And while many patients are familiar with these movements I am continually amazed at how few people do these the right way.
So let’s look at how to do these pelvic tilts the right way.

Starting Positions For Acute Low Back Pain
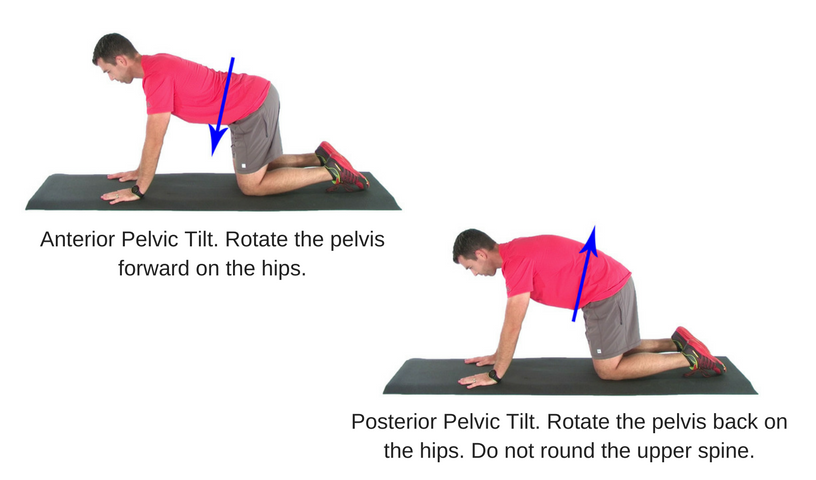
While pelvic tilts can be done in several positions, the non-weight bearing positions of supine/hook lying and quadruped are the best starting exercises for most acute low back pain patients. These postures minimize compression on the spine, but also minimize muscle tension around the hips, making it easier to rotate the pelvis. (Note: As soon as the patient is able pelvic tilts can also be done in additional postures to set up the next phases of the rehab program. See discussion below.)
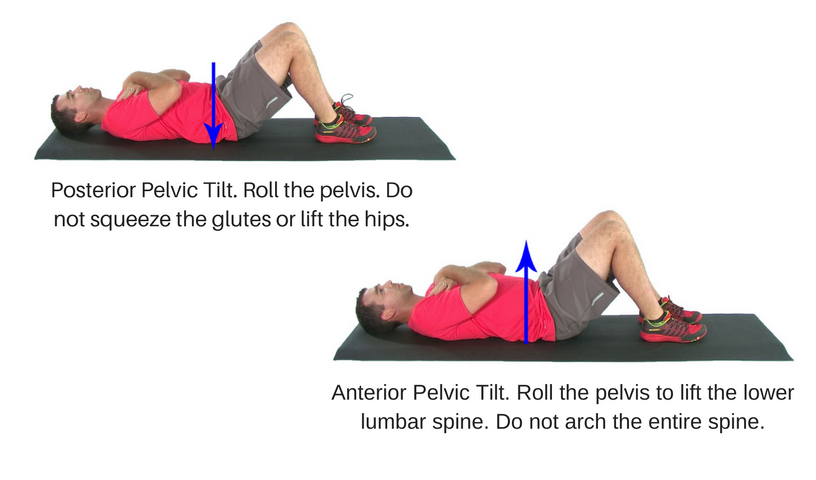
Anterior Pelvic Tilt
An anterior pelvic tilt is associated with nutation of the sacrum, increased lumbar lordosis, and relative flexion of the hips. To ensure proper form instruct the patient to gently roll the pelvis forward. From a supine position they are trying to lift the lower spine away from the floor. In the quadruped position they can visualize the pelvis rotating forward on their hip joints. A spine model helps with this visualization.
It is extremely common with low back pain patients to have difficulty performing an anterior pelvic tilt properly. Most commonly there will be a lack of lower lumbar movement into extension with under activity of the multifidus (and probably the psoas). Instead the patient is more likely to initiate the motion from the thoracolumbar erectors. This is evidenced but a thrusting of the anterior pole of the thorax forward instead of a rolling motion centered at the lower lumbar spine and sacral base. To prevent this be sure the patient focuses on using the deep muscles in the lowest aspect of their spine to drive the motion.
Posterior Pelvic Tilt
A posterior pelvic tilt is associated with the combined motions of sacral counternutation, lumbar flexion, and relative hip extension. Instruct the patient to gently roll the pelvis back to flatten the spine. From a supine position they are trying to press the lower spine towards the floor. In the quadruped position they can visualize the tucking the pelvis under the spine.
When done correctly it is the lower abdominals, pelvic floor, and obturator group (including the piriformis) that should drive the motion. However, it is not uncommon for patients to rely on the glutes and/or hamstrings for this motion.
In addition to palpating a strong glute contraction the tendency will be for the hips to lift off the table. In some cases there will also be a dominance of the upper abdominals over the lower abdominals. With these patients you will see a total flexion of the spine as opposed to a focal flexion contained at the lower lumbar spine.
And remember, with both the anterior and posterior tilts this is not, and should not be a big movement. It is much more about control than range. It is important to convey this to the patient.
A Primer For Future Exercise
Control of lumbo-pelvic posture is a critical movement skill. This makes pelvic tilt exercises a critical exercise not only for acute low back pan, but for virtually any low back pain patient.
Think about it. A common goal with virtually all of our back pain patients is to ensure spine stability. In other words, to control the posture and position of the spine during movement. This comes back to the ability to control of lumbo-pelvic posture and movement.
Excessive lumbar flexion with forward bending or sitting? That’s a lack of control of the anterior pelvic tilt position. Compensatory lumbar hyper-extension with gait or upright posture? That a deficiency in posterior pelvic tilt control.
So when the goal is to stabilize the spine, it only makes sense to develop isolated lumbo-pelvic control before prescribing more complex movements that require this control.
Seated Pelvic Tilt
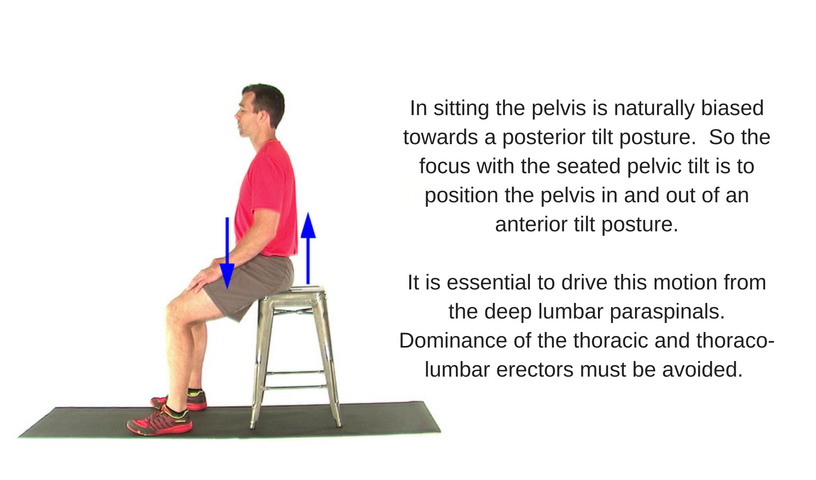
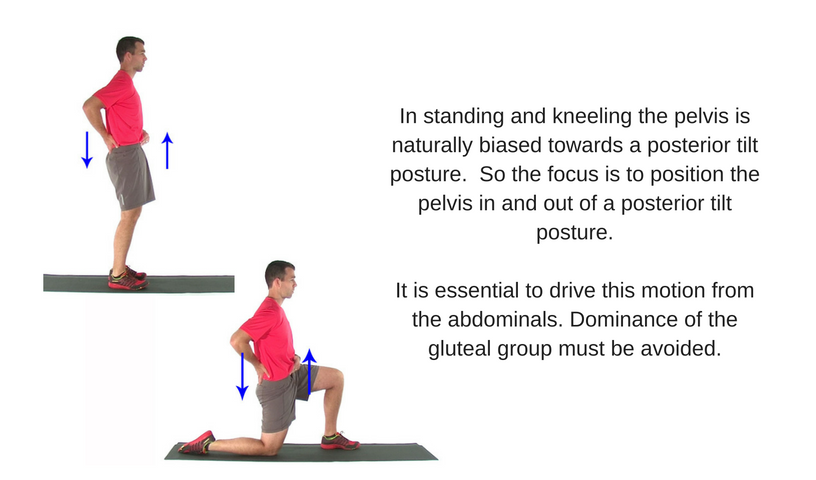
Pelvic Tilts In An Upright Posture