
Muscle imbalances are a common cause of neck pain. As such, clinicians need simple and effective tests to assess movement and muscle balance in the cervical spine. And they need to know what to do when dysfunction in uncovered.
That has been the topic of this three part article series. Neck flexion and neck extension were the topics of the first two articles. In this final article we will discuss assessment and corrective exercise recommendations for the cervical rotators.
Basic Anatomy of the Cervical Rotators
As discussed in parts one and two of this series, the cervical musculature can be divided into intrinsic and extrinsic muscles. The intrinsic rotators include the rectus capitus posterior major, the oblique capitus superior and inferior, and the splenius group. These muscles are well suited to produce pure cervical rotation about a vertical axis.
The extrinsic cervical rotators include the sternocleidomastoids (SCM), scalenes, Levator Scapulae, and Upper Trapezius. Due to their orientation these muscles are unable to produce pure rotation about the vertical axis. Instead, rotation will occur in conjunction with lateral flexion or extension. These accessory motions will compromise cervical stability and control.
Under normal circumstances these intrinsic and extrinsic muscles work synergistically. But with many neck, thoracic, and shoulder conditions it is common for the extrinsic muscles to become dominant over the intrinsic extensors. As clinicians we must be able to decipher these imbalances. And we must know what to do when we find them.
Assessment of Cervical Rotator Muscle Imbalance
Muscle balance of the cervical rotators can be assessed with active cervical rotation range of motion (ROM). This is best done from a seated or standing position (although it can be done in quadruped as well). As you observe the patient actively rotate their neck you need to look for two things.
First, what is the range? How far can the patient comfortably turn their neck to each side? Under normal circumstances the patient should be able to turn 90 degrees (or very close to it). This motion should be pain free and symmetrical to each side.
Second, what is the quality of the motion? Ideally the neck should rotate around a vertical axis. And each segment should contribute to this motion. (That does not mean each segment should rotate to the same degree. The upper cervical spine will rotate more than the lower. But each segment should contribute to the motion).
When the extrinsic rotators are dominant over the intrinsics the neck will often laterally flex and/or extend as it rotates. This is an undesirable compensatory pattern that can create excessive stress, tissue damage, and eventually pain.
Cervical Rotator Exercises
Faulty active cervical rotation is an indication of cervical rotation dysfunction. The exercises that follow are two simple progression to help correct this problem.
But before jumping into prescribing cervical rotation exercises make sure cervical flexion and extension is functional (see part 1 and part 2 of this article series). When cervical rotation is dysfunctional imbalances will often be found in flexion and/or extension as well. In many cases correcting these flexion or extension imbalances will also clear the rotation dysfunction.
Supine Neck Retraction with Rotation
The key to re-training cervical rotator muscle balance is to teach the patient to rotate the cervical spine around a vertical axis without the compensatory muscles dominating the motion. This first exercise is one of the best ways to do this.
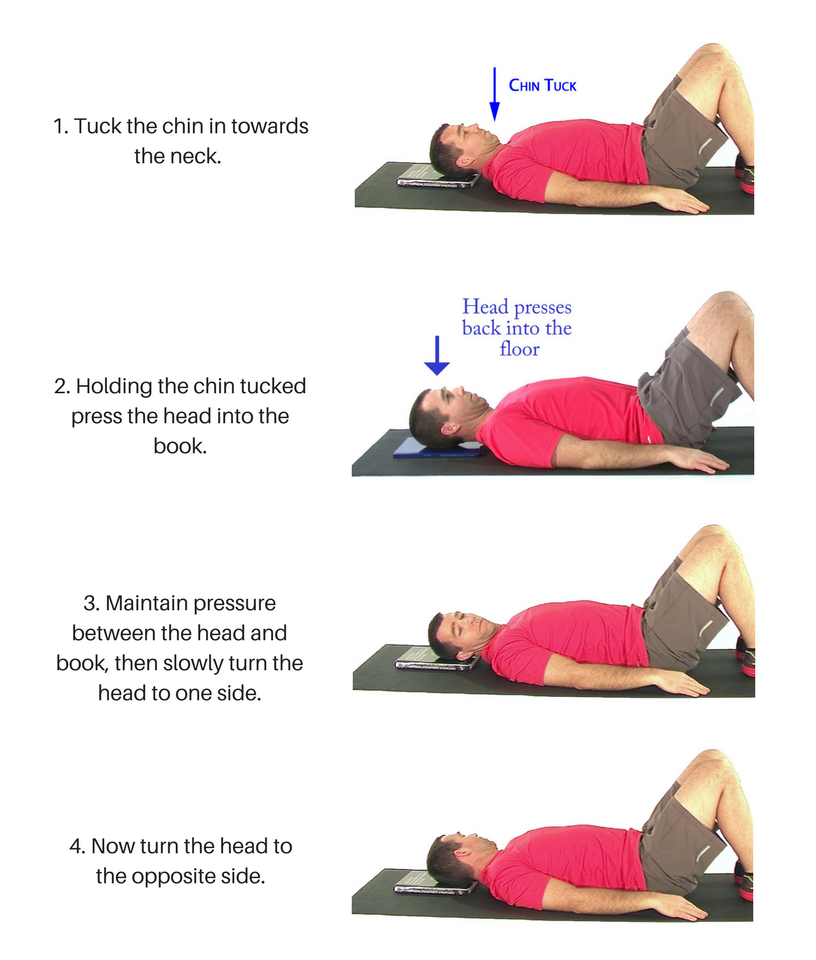
Begin in a hook lying position. Have the patient tuck their chin in towards their neck. Then gently press the back of the head into the book. The chin must remain tucked as they do this. This will engage the deep neck flexors and intrinsic cervical extensors / rotators. While holding the chin tucked and maintaining gentle pressure against the book the patient slowly rotates their head to one side.
Proper form is critical. It is important that the neck does not bend to the side as it rotates. The patient should also visualize the head and neck rotating around a straight rod running from the top of their head down through the center of cervical spine as they move.
Don’t Engage the Extrinsic Muscles
It is also important that the extrinsic muscles do not contract. We want to ensure the patient is using the intrinsic rotators to drive the motion. The patient can be taught to palpate the SCM muscles just above the sternal notch with the movement. This can provide a valuable source of feedback as to the success of the motion. The patient should be instructed to rotate as far as possible without pain or the SCM muscles contracting. I typically have my patients perform 10-15 repetitions to each side.
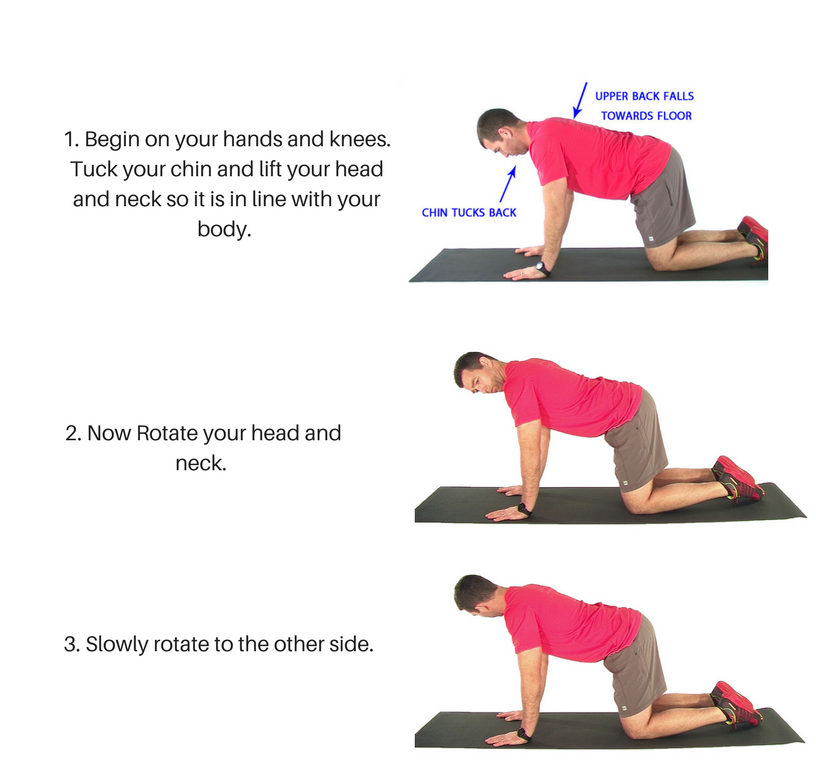
Quadruped Neck Rotation
This next exercise shifts to the quadruped position. Make sure the shoulder blades are relaxed and the thoracic and lumbar spines are in a neutral posture. From this position tuck the chin towards the neck, then gently extend the head back towards the ceiling. This extension should come from the lower neck and upper thoracic spine. It is not a big movement. It is more about bringing the neck back to neutral.
In this posture the Levator Scap and Upper Trap must be relaxed. It is the intrinsic cervical extensors that must hold the cervical spine in neutral alignment (see previous article).
From this position gently rotate the head and neck to one side. This rotation should occur about a vertical axis. There must not be any lateral flexion or additional extension with the movement. And the Levator Scapulae and Upper Trap must not kick in as the neck rotates. The clinician can palpate the muscles to check this during the movement.
Unlike the previous exercise where the book helped to guide the rotation, the patient must learn to feel for the proper motion. The clinician may need to provide feedback to the patient to get this right.
Again the movement should be slow and easy. As the range of rotation increases the patient will feel the extrinsic muscles kick in. They should avoid this outer range in the initial stages of the exercise. Start with 10-15 repetitions to each side. Focus on quality.